SOCIAL MEDIA
Portuguese Medical Association's Scientific Journal

Introduction: Acute primary angle closure attack is an ophthalmological emergency. The aim of this study was to describe the cases diagnosed in the Emergency Department, by correlating the initial complaint with the Manchester triage level and ultimately the time needed until ophthalmological evaluation and iridotomy.
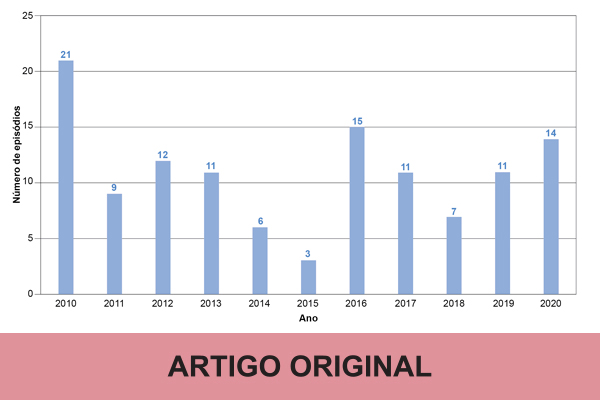
Material and Methods: Retrospective analysis of the electronic medical records of patients with acute primary angle closure attack that attended the Ophthalmology Emergency Department of our tertiary center between January 2010 and December 2020. Overall, 2228 Emergency Department episodes coded with the diagnoses glaucoma or ocular hypertension were retrieved, followed by screening of each episode for correct identification of true acute primary angle closure attacks. Clinical data was gathered, including Manchester triage level, presenting complaint, intraocular pressure at presentation, first medical specialty that observed the patient, time until observation by Ophthalmology and time until laser iridotomy.
Results: Among the 120 patients identified, 84 (70%) were female and the mean age was 68 ± 12 years. Mean intraocular pressure at admission was 53.4 ± 12.4 mmHg, and 9.2% of patients presented only non-ocular complaints, while 9.2% presented mixed complaints (ocular and non-ocular). Most patients (68.1%) with only non-ocular or mixed complaints were triaged to a non-ophthalmologist (p < 0.001). Concerning the triage system, at admission, most patients (66.7%) were labelled yellow (urgent), while 9.2% and none were labelled as orange (very urgent) or red (emergent), respectively. Most patients (83.3%) were directly sent to Ophthalmology (properly triaged), while the remaining were incorrectly assigned to a non-ophthalmologist. Median time until observation by Ophthalmology was 49 minutes in the properly triaged group (min. 15, max. 404), while it was 288 minutes (min. 45, max. 871) in those who were incorrectly triaged (p < 0.001). Likewise, median time until treatment with laser iridotomy was 203 minutes in the properly triaged group (min. 22, max. 1440) and 353 minutes in the incorrectly triaged group (min.112, max. 947) (p < 0.001).
Conclusion: Most patients with acute primary angle closure attack were not properly triaged according to the level of the Manchester triage system. There was a significant delay in the diagnosis and treatment of those patients who were first assigned to non-ophthalmologists. There is a need to raise awareness regarding the presenting signs and symptoms of an acute primary angle closure attack in order to avoid preventable vision loss.