SOCIAL MEDIA
Portuguese Medical Association's Scientific Journal

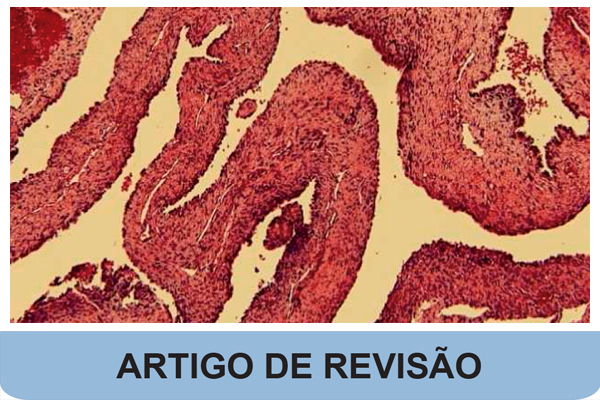
Congenital pulmonary airway malformations (CPAMs), according to the Stocker classification, comprise five types, two of which are non-cystic in nature (types 0 and 3) whereas the others present as cystic lung lesions (types 1, 2 and 4). While there is consensus that symptomatic lesions should be managed surgically, the asymptomatic cases are more problematic in terms of therapeutic intervention. The dilemma is further complicated by CPAM types 1 and 4 and their preneoplastic potential. In the case of CPAM type 1, there are reports of lipidic adenocarcinoma arising from the mucinous component. Type 4 has been equated to type I or cystic pleuropulmonary blastoma (PPB), a proposition that has been challenged in the past. Pleuropulmonary blastoma is associated with a heterozygous germline or somatic variants in DICER1. It was recognized that the earliest stage of the sarcomatous progression of PPB was a multicystic lesion in the periphery of the lung whose architectural features were identical to CPAM type 4. This narrative review addresses key aspects of the pathogenetic and diagnostic issues of type I PPB/CPAM type 4, as well as the association of DICER1 and PPB, offering valuable insights for pediatricians and clinicians caring for young adults who are impacted by the presence of a germline DICER1 variant.